

Introduction: The clonal hematopoiesis with somatic mutations is age-related phenomenon with a frequency around 10% for population older than 65 years in contrast to population younger than 50 years with frequency of 1%. Mutations in genes involved in epigenetic modification and RNA splicing, which are recurrently mutated in myeloid neoplasms and associated with increased risk of hematologic cancer, seem to represent a premalignant condition. Generally, ASXL1 mutations are frequently found in myeloid malignancies. Patients with chronic myeloid leukemia (CML) diagnosed at the age of 15 to 39 years, also called adolescent and young adults (AYAs), have a worse prognosis and response to tyrosine kinase inhbitors (TKIs) compared to elderly patients. Little is known about the molecular background differing AYA from the common group of CML patients.
Objectives: To determine, whether the worse prognosis and response to therapy of CML AYAs is associated with the clonal hematopoiesis with somatic mutations.
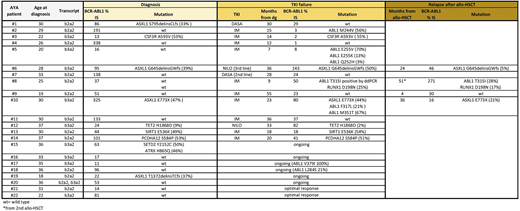
Methods: Samples from 22 AYAs were retrospectively analyzed at the time of diagnosis (aged 18-37; Table 1). Of them, 20 patients failed on TKI or relapsed after allo-HSCT (allogeneic hematopoietic stem cells transplantation). In 6/20 AYAs, mutations in the kinase domain of BCR-ABL1 were detected at the time of TKI failure (M244V, T315I, E255K/V + Q252H, F317L + M351T, V379I, L284S). Two responders were included for comparison. Sequencing of custom myeloid panel (Roche), partly or fully covering 36 genes frequently mutated in myeloid malignancies, was performed on MiSeq (Illumina). Data was analyzed in NextGENe software (Softgenetics). The detected variants were characterized by open-source databases (VarSome, Ensembl, COSMIC, NCBI - dbSNP) and confirmed by Sanger sequencing and/or ASO-ddPCR.
Results: At the time of diagnosis, somatic mutations were identified in ASXL1 (n=4), CSF3R (n=1), TET2 (n=1), PCDHA12 (n=1), SETD2 (n=1), ATRX (n=1), and SIRT1 (n=1) in 10/20 AYAs, who subsequently failed on treatment (Table 1). Overall, 6 missense, 3 frameshift mutations and one nonsense mutation were detected. In patients #21 and #22 with optimal response to TKIs, no mutations were detected at diagnosis. In patient #10, ASXL1 mutation E773X was confirmed at the time of TKI failure and also at the allo-HSCT relapse. In patient #6, G645delinsGWfs was found at the diagnosis and on the 3rd line nilotinib treatment. Another ASXL1 mutation, S795delinsCLfs, was found in a patient #1 only at diagnosis. In patient #19, ASXL1 mutation T1372delinsTCfs found at diagnosis will be followed during the TKI treatment. In patient #3, the CSF3R mutation A593V was found at diagnosis and confirmed 14 months after the imatinib initiation. In patient #8, who relapsed after 2nd allo-HSCT, the RUNX1 D198N was found in the same clone bearing BCR-ABL1 T315I, both confirmed by ASO-ddPCR also before 1st allo-HSCT. This clone was, in the follow-up treatment, responsible for the relapse to CNS and also the relapse even after 3rd allo-HSCT and patient died.
Conclusions:
The preliminary data of this work outlined that somatic mutations in the myeloid genes are frequently found in CML AYAs, who failed on the TKI or relapsed after allo-HSCT, alone or together with mutated BCR-ABL1. The most frequently mutated gene was ASXL1, which is in line with the work by Ernst et al. (2018) even though on younger patients including children. Despite the clonal hematopoiesis with somatic mutations is considered as age-related phenomenon, in AYA CML patients, it may represent a critical problem in achieving sustained molecular response on solo TKI therapy, or even worse, it may result in higher risk of therapy failure and disease progression.
Supported by MZCR 00023736
Stoklosa:Janssen: Honoraria. Machova:Incyte: Consultancy; Angelini: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal